What to do if the implant is too close to the adjacent tooth?

Someone sent me this question not too long ago, with the accompanying photo and instantly I sympathized with the sender.
I too have found myself–or I mean, my implant –in this position
And it is not fun.
From the outside looking in, it is easy to cast opinions. Keyboard warriors are at large these days. But anyone who has placed any volume of implants will have run into this situation at one time or another. It is a requisite rite of passage for a budding implantologist.
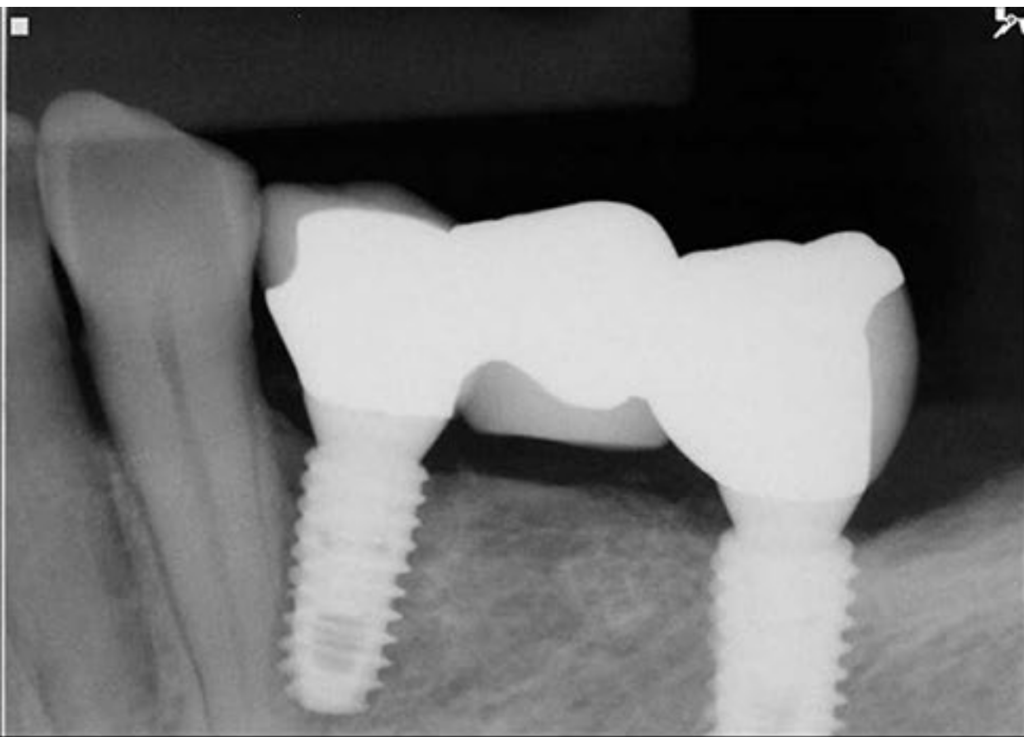
The implant was placed 0.8mm away from the adjacent tooth. Lots of questions you might have:
- Is it doomed to fail?
- What’s the prognosis here?
- Any examples of success with an implant this close to the adjacent tooth?
- What are the appropriate next steps?
So let’s dig in.
Anecdotal Suggestion
While this situation can be super stressful, it doesn’t necessarily mean disaster.
Anecdotally, I have at times, and many others have placed implants closer than we wish we would have to adjacent teeth. It’s happened once or twice. And aside for a few sleepless nights, I (and the patient) have had zero issues from it.
Literature
Long term clinical result of implant induced injury on the adjacent tooth
A study that followed patients for over 10 years found that even when implants directly injured nearby teeth, 90.6% of those teeth remained functional long-term. Out of 32 implants, only a few needed root canal treatment, and one implant failed in cases with direct root invasion.
Only 3 of the teeth needed to be extracted. And 7 of the teeth ended up having endodontic treatment. However, 90.6% of the teeth remained functional.
Also, the implant survival rate was high at 96.9%, and the stability even improved over time. So, immediate extraction isn’t typically needed, and the implant can still integrate well. Link
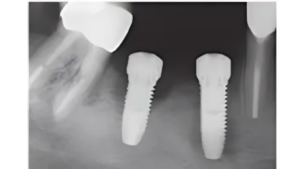
Here’s a photo from the study:
Appropriate Next Steps?
In my humble opinion, the first thing is to take a step back and not stress too much. Things will most likely be just fine.
Now, here are some potential options:
- Option A: Take the implant out and re-do the implant placement. You still have time if you want to do this. This is still a viable option. I have done this a handful of times after stewing over my implant positioning for a few days. I’ve called the patient back and repositioned it.
- Yes, it does feel stressful to explain to the patient why you want to redo it
- Consider if you believe this will make the patient better or worse off
- Option B: Leave it as is, and monitor the adjacent tooth closely for any pulpal changes. (You might be surprised to find that nothing happens.)
Note: You will likely have unideal soft tissue next to that adjacent tooth. Careful management would be advised.
Honestly, in this situation, to me it does not look like there is a clear right or wrong. There is no negligence here. You did the best you could. Now navigate what you feel would be best for you and the patient.
Hope that helps.
Don’t stress.
Ivan
Responses
@jostanger @drcajee @87madrigal @mickyfrick I’d love to hear your any insight you have into these types of situations. They’re no fun, but many of us have found ourselves here!
This just happened to me last week. An implant (lateral… usually always the laterals) I placed was too close to an adjacent tooth, and while it’s not ideal, it’s something we can manage. It was an immediate post extraction so it got deviated by the socket. In that case, I removed the implant and redirected it to the correct position without long-term complications.
In my experience, implants placed too close to adjacent teeth can still have good outcomes in many cases, especially if it’s just the apical portion, but it’s not the standard we aim for. It can affect bone stability or lead to challenges with the adjacent tooth over time. Guided surgery is an excellent tool to help us avoid these situations, but in the real world, things don’t always go perfectly. When it does happen, the focus should be on identifying the issue early and taking steps to ensure the best possible outcome for the patient.
I completely agree with your reasoning here. If you feel like you can do better, you owe yourself and the patient the opportunity to do so.
I also have the pleasure of seeing a lot of implants placed by a lot of people— and sometimes compromised tx still works and has no issues. Always inform the patient though about the situation!
I agree 100 percent
thanks for chiming in @drgene1